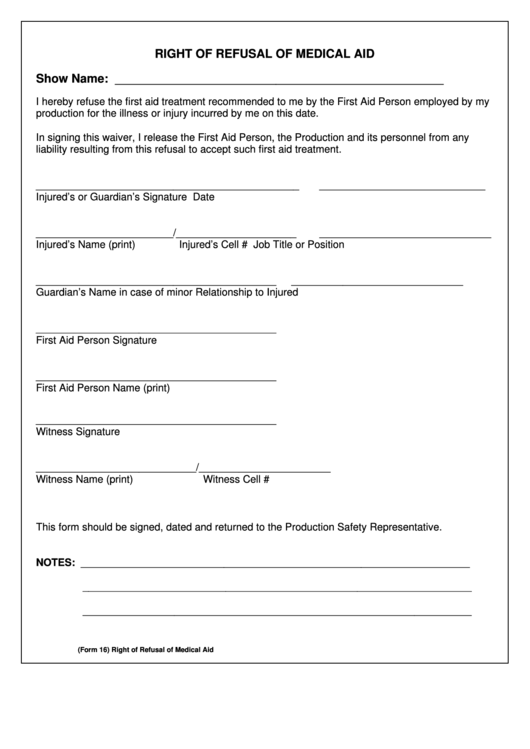
Refusal Form - This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by. ____________________ from any and all liability. “i am refusing to have these radiographs taken at this time. In this circumstance, consider asking the patient to sign. A record of the patient’s refusal of the treatment/testing plan or advice. _____________________________________________ i am provided with this refusal form and information so i may understand the recommended treatme. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could.
A record of the patient’s refusal of the treatment/testing plan or advice. “i am refusing to have these radiographs taken at this time. This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by. In this circumstance, consider asking the patient to sign. _____________________________________________ i am provided with this refusal form and information so i may understand the recommended treatme. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could. ____________________ from any and all liability.
“i am refusing to have these radiographs taken at this time. A record of the patient’s refusal of the treatment/testing plan or advice. _____________________________________________ i am provided with this refusal form and information so i may understand the recommended treatme. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could. In this circumstance, consider asking the patient to sign. ____________________ from any and all liability. This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by.

Medical Treatment Refusal Form Template amulette
____________________ from any and all liability. _____________________________________________ i am provided with this refusal form and information so i may understand the recommended treatme. In this circumstance, consider asking the patient to sign. This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by. By signing below, i understand that.
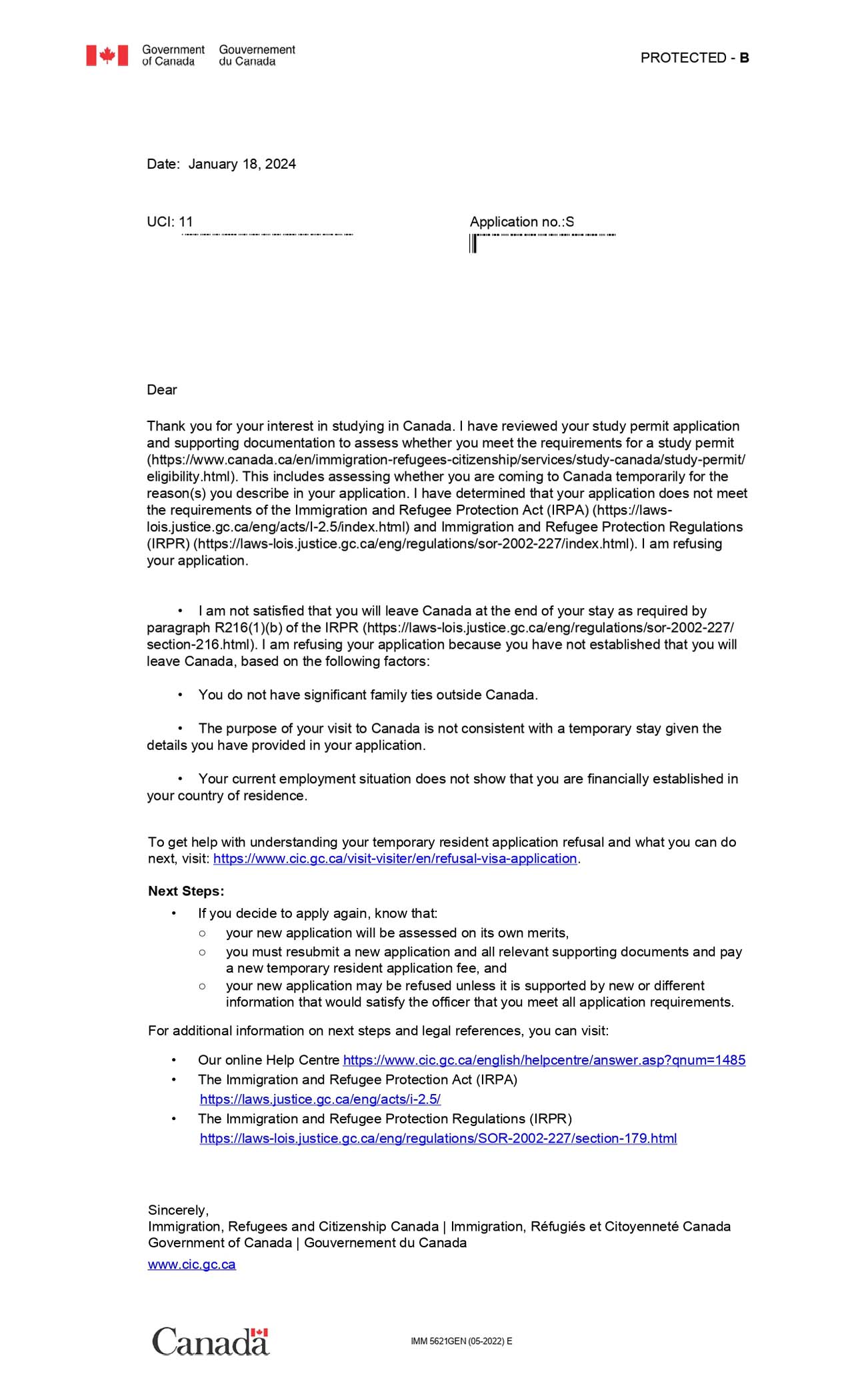
Canada Visa Refusal Immigration Refusal Lawyers
In this circumstance, consider asking the patient to sign. This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by. ____________________ from any and all liability. “i am refusing to have these radiographs taken at this time. A record of the patient’s refusal of the treatment/testing plan or advice.
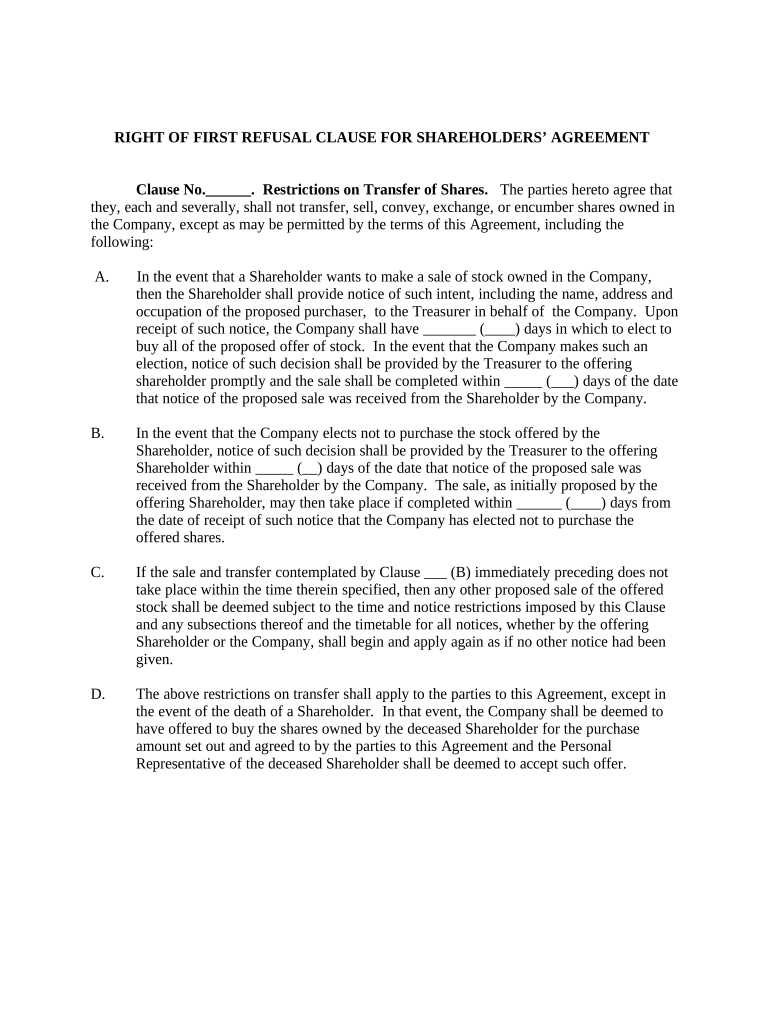
First Refusal Complete with ease airSlate SignNow
____________________ from any and all liability. _____________________________________________ i am provided with this refusal form and information so i may understand the recommended treatme. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could. A record of the patient’s refusal of the treatment/testing plan or advice. In this circumstance, consider asking the.
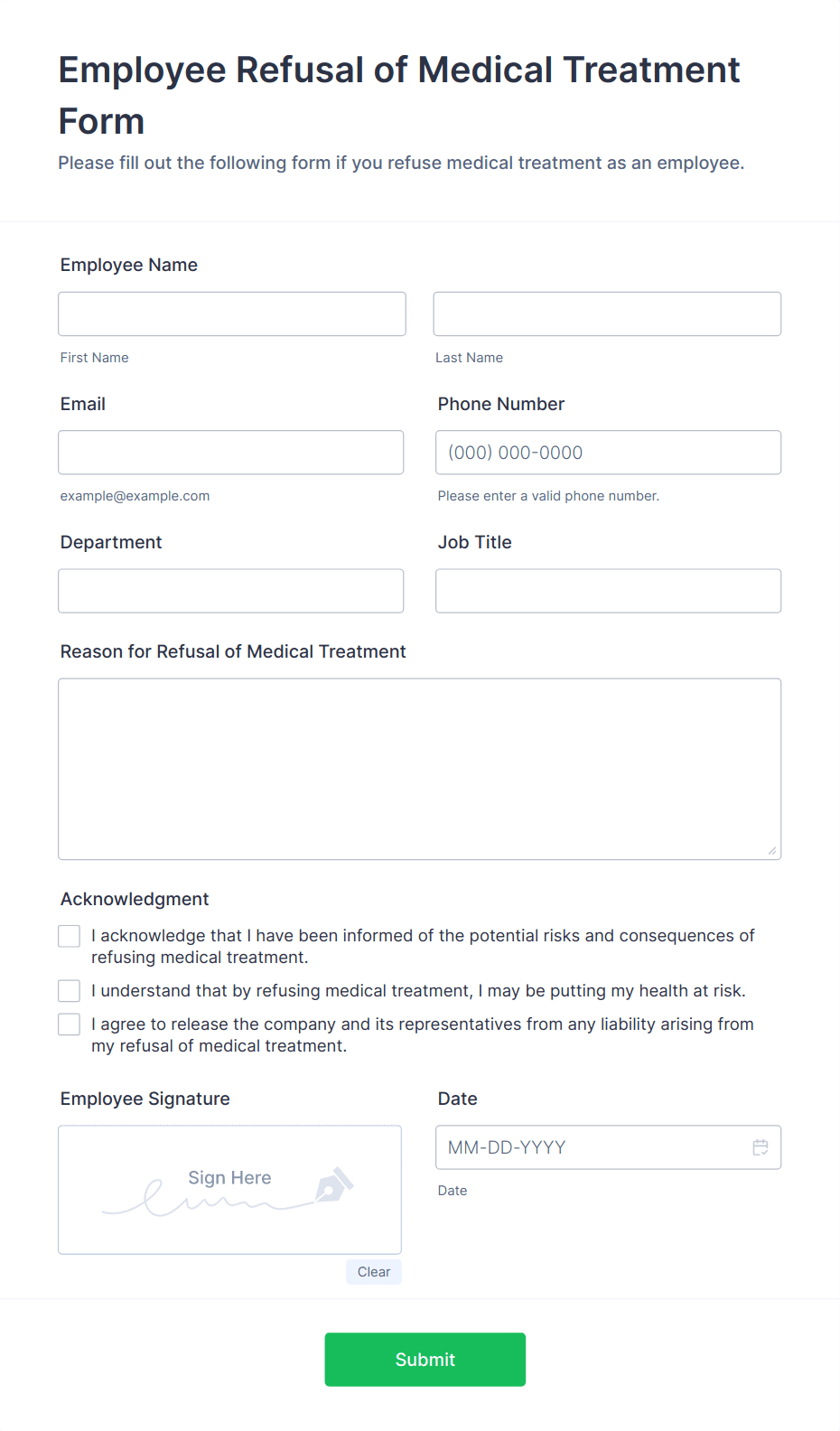
Employee Refusal of Medical Treatment Form Template Jotform
____________________ from any and all liability. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could. “i am refusing to have these radiographs taken at this time. In this circumstance, consider asking the patient to sign. This form should be signed by the patient or authorized party if he/she refuses any.

Medical Treatment Refusal Form Template amulette
_____________________________________________ i am provided with this refusal form and information so i may understand the recommended treatme. This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could. A record.

Informed Refusal Form Edit & Share airSlate SignNow
This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by. A record of the patient’s refusal of the treatment/testing plan or advice. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could. _____________________________________________ i am provided with this refusal.

Vaccine Refusal Form Template Jotform
In this circumstance, consider asking the patient to sign. A record of the patient’s refusal of the treatment/testing plan or advice. “i am refusing to have these radiographs taken at this time. ____________________ from any and all liability. _____________________________________________ i am provided with this refusal form and information so i may understand the recommended treatme.
Waiver Of Right Of First Refusal Template
By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could. ____________________ from any and all liability. This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by. In this circumstance, consider asking the patient to sign. A record of the.
Refusal of Medical Treatment Media Services Fill Out and Sign
“i am refusing to have these radiographs taken at this time. _____________________________________________ i am provided with this refusal form and information so i may understand the recommended treatme. ____________________ from any and all liability. A record of the patient’s refusal of the treatment/testing plan or advice. In this circumstance, consider asking the patient to sign.

Refusal of treatment form pdf Fill out & sign online DocHub
“i am refusing to have these radiographs taken at this time. A record of the patient’s refusal of the treatment/testing plan or advice. _____________________________________________ i am provided with this refusal form and information so i may understand the recommended treatme. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could. ____________________.
In This Circumstance, Consider Asking The Patient To Sign.
A record of the patient’s refusal of the treatment/testing plan or advice. “i am refusing to have these radiographs taken at this time. This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by. _____________________________________________ i am provided with this refusal form and information so i may understand the recommended treatme.
____________________ From Any And All Liability.
By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could.