Medicare Reconsideration Form - Your next level of appeal is a. Submission of the information requested on this form is voluntary,. The information provided will be used to further document your appeal. Transferring your appeal rights to your provider or supplier so they can file an appeal if medicare decides not to pay for an item or service. Anyone who misrepresents or falsifies essential information requested by this form may upon conviction be subject to fine or. Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal.
Submission of the information requested on this form is voluntary,. Your next level of appeal is a. Transferring your appeal rights to your provider or supplier so they can file an appeal if medicare decides not to pay for an item or service. Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. Anyone who misrepresents or falsifies essential information requested by this form may upon conviction be subject to fine or. The information provided will be used to further document your appeal. If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal.
If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. The information provided will be used to further document your appeal. Anyone who misrepresents or falsifies essential information requested by this form may upon conviction be subject to fine or. Your next level of appeal is a. Transferring your appeal rights to your provider or supplier so they can file an appeal if medicare decides not to pay for an item or service. Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. Submission of the information requested on this form is voluntary,.
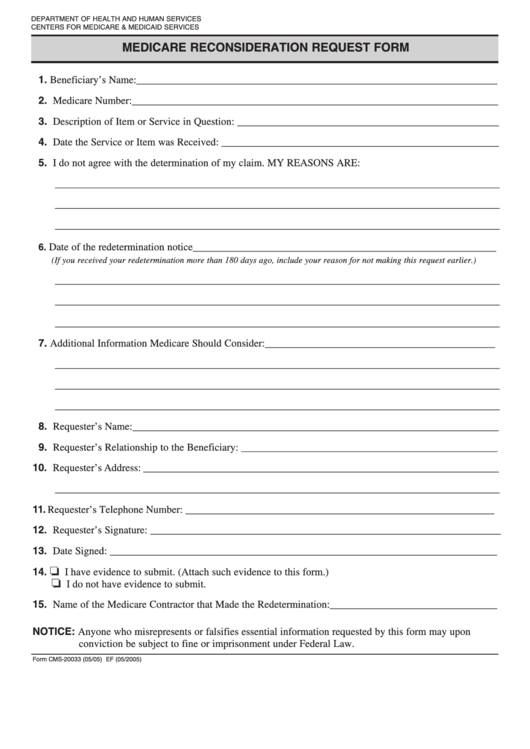
Fillable Medicare Reconsideration Request Form printable pdf download
If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. Anyone who misrepresents or falsifies essential information requested by this form may upon conviction be subject to fine or. The information provided will be used to further document your appeal. Transferring your appeal rights to your provider or supplier so.

Fillable Online How to complete the Medicare reconsideration request
The information provided will be used to further document your appeal. Transferring your appeal rights to your provider or supplier so they can file an appeal if medicare decides not to pay for an item or service. Anyone who misrepresents or falsifies essential information requested by this form may upon conviction be subject to fine or. Please attach the evidence.
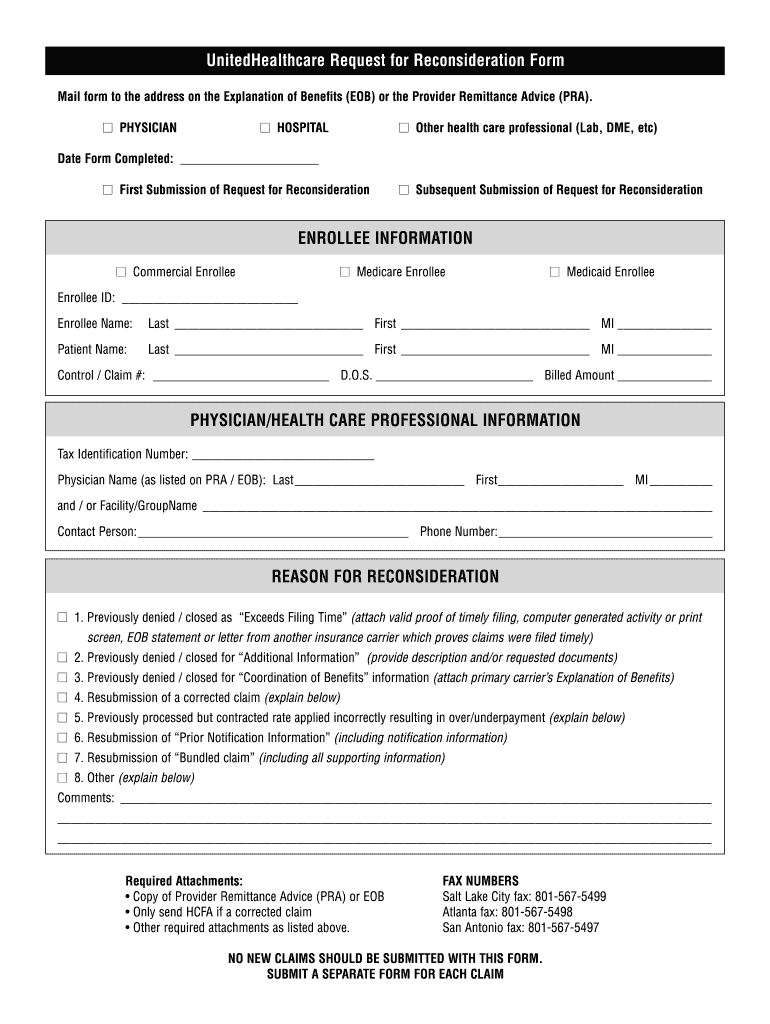
Community First Health Plan Appeal Form
Anyone who misrepresents or falsifies essential information requested by this form may upon conviction be subject to fine or. Your next level of appeal is a. Submission of the information requested on this form is voluntary,. Transferring your appeal rights to your provider or supplier so they can file an appeal if medicare decides not to pay for an item.
What Is A Medicare Enrollment Center
The information provided will be used to further document your appeal. Anyone who misrepresents or falsifies essential information requested by this form may upon conviction be subject to fine or. Your next level of appeal is a. Submission of the information requested on this form is voluntary,. Please attach the evidence to this form or attach a statement explaining what.
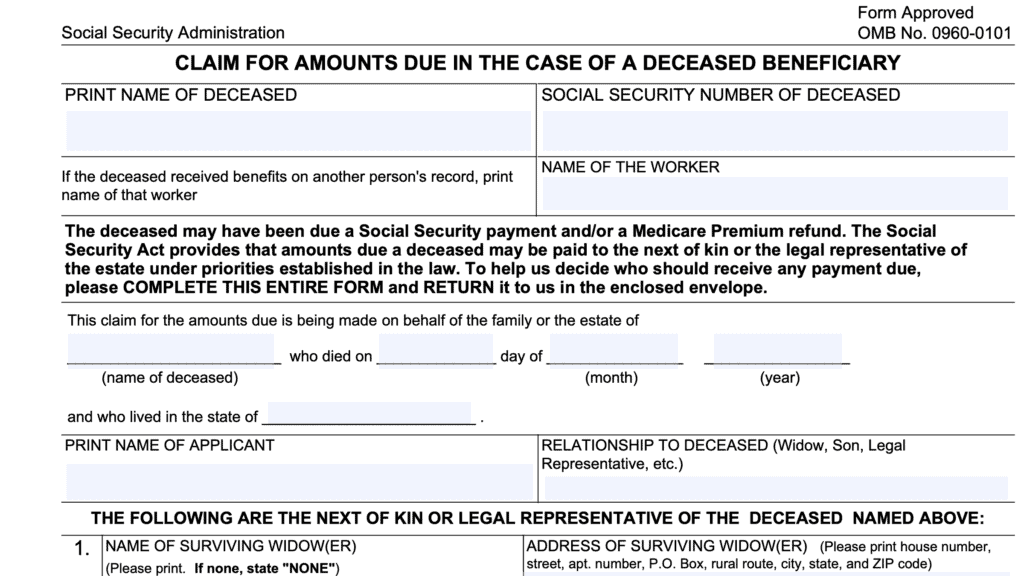
Ssa 44 2025 Medicare Irmaa Appeal Form Zachary Rami
Submission of the information requested on this form is voluntary,. If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. Transferring your appeal rights to your provider or supplier so they can file an appeal if medicare decides not to pay for an item or service. Your next level of.
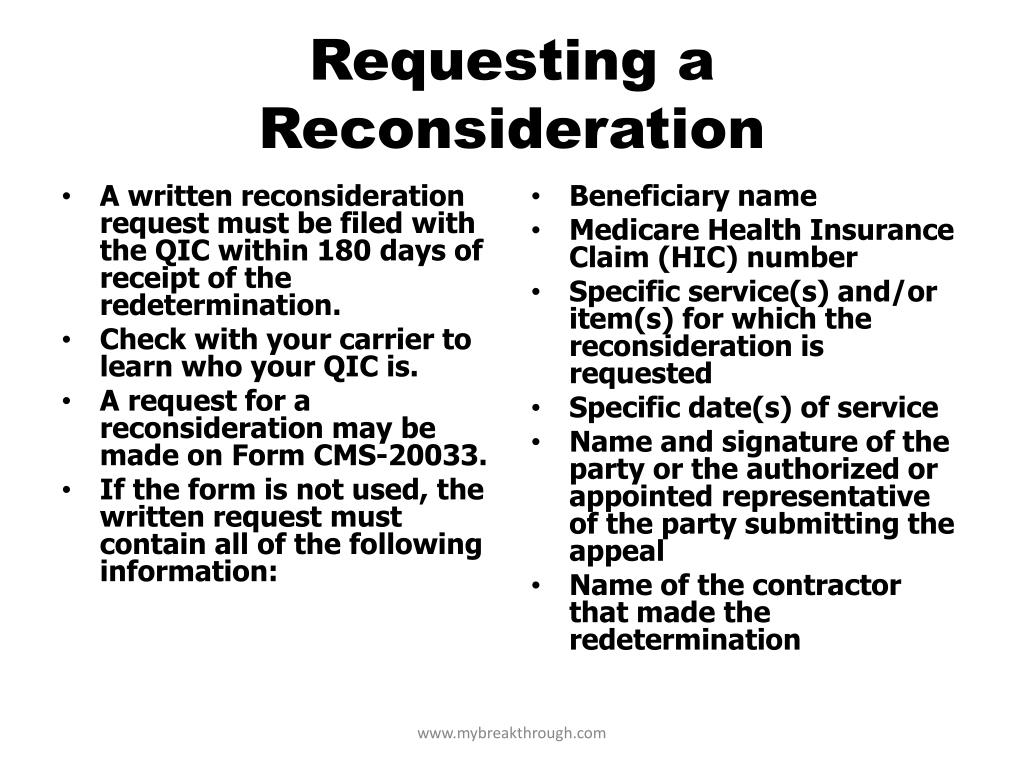
PPT The Medicare Appeals Process PowerPoint Presentation, free
Transferring your appeal rights to your provider or supplier so they can file an appeal if medicare decides not to pay for an item or service. Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. The information provided will be used to further document your.

PPT The Medicare Appeals Process PowerPoint Presentation, free
Transferring your appeal rights to your provider or supplier so they can file an appeal if medicare decides not to pay for an item or service. Anyone who misrepresents or falsifies essential information requested by this form may upon conviction be subject to fine or. If you received a medicare redetermination notice (mrn) on this claim do not use this.

Medicare Part B JF Redetermination Form PDF
Submission of the information requested on this form is voluntary,. The information provided will be used to further document your appeal. If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. Transferring your appeal rights to your provider or supplier so they can file an appeal if medicare decides not.

Medicare Redetermination Form 2020 2020 Fill and Sign Printable
Anyone who misrepresents or falsifies essential information requested by this form may upon conviction be subject to fine or. The information provided will be used to further document your appeal. Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. Submission of the information requested on.
PPT THE MEDICARE APPEALS PROCESS PowerPoint Presentation, free
Submission of the information requested on this form is voluntary,. If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. Your next level of appeal is.
Submission Of The Information Requested On This Form Is Voluntary,.
Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. Transferring your appeal rights to your provider or supplier so they can file an appeal if medicare decides not to pay for an item or service. Your next level of appeal is a.
The Information Provided Will Be Used To Further Document Your Appeal.
Anyone who misrepresents or falsifies essential information requested by this form may upon conviction be subject to fine or.