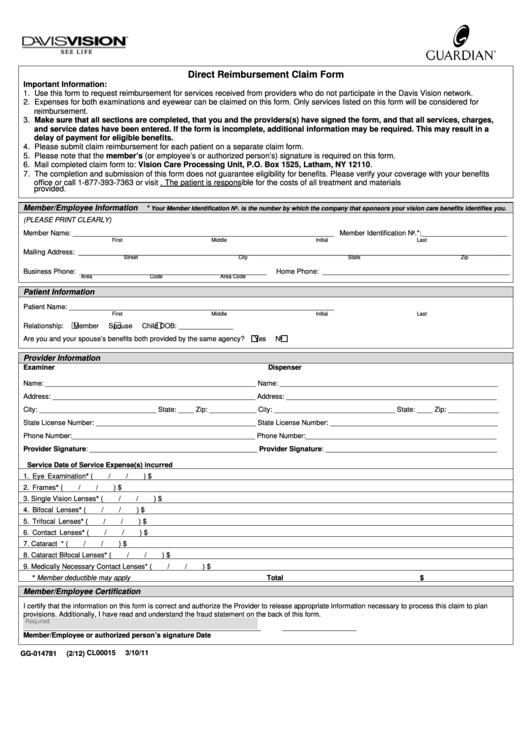
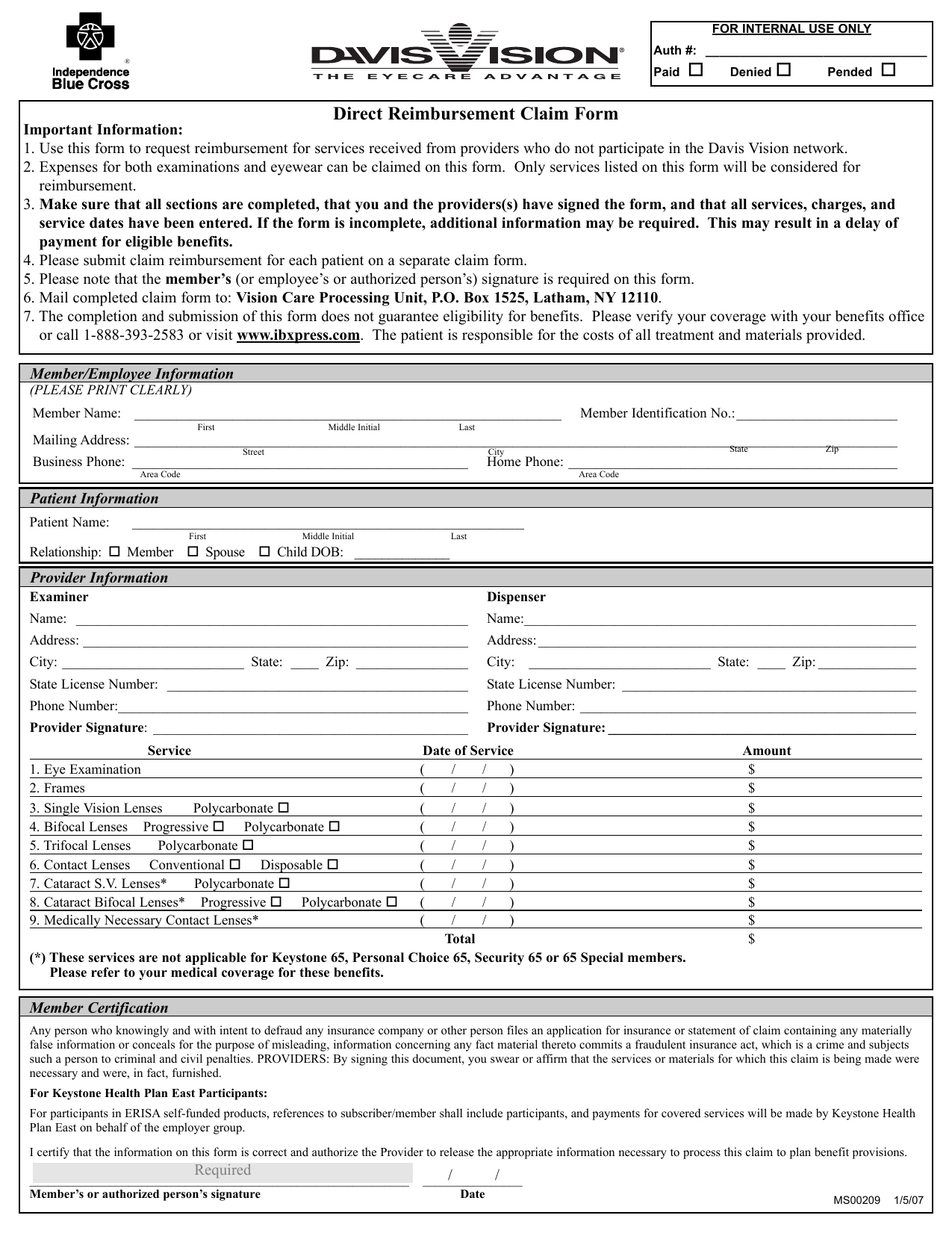
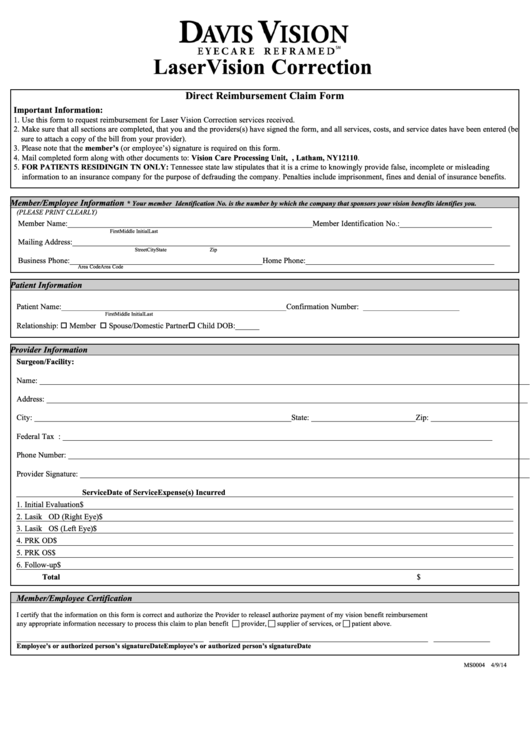
Davis Vision Claim Form - Please submit claim reimbursement for each patient on a separate claim form. Box 1525, latham, ny 12110. Please note that the member’s (or employee’s or authorized person’s). Mail completed claim form to: In new hampshire, any person who, with a purpose to injure, defraud, or deceive any insurance company, files a statement of claim containing any false,. Use this form to request reimbursement for services received from providers who do not participate in the davis vision. The completion and submission of this form does. Vision by metlife member reimbursement form to request reimbursement, complete and print this form, enclose a legible copy of your itemized. Vision care processing unit, p.o.
Box 1525, latham, ny 12110. The completion and submission of this form does. Vision care processing unit, p.o. In new hampshire, any person who, with a purpose to injure, defraud, or deceive any insurance company, files a statement of claim containing any false,. Please submit claim reimbursement for each patient on a separate claim form. Vision by metlife member reimbursement form to request reimbursement, complete and print this form, enclose a legible copy of your itemized. Mail completed claim form to: Use this form to request reimbursement for services received from providers who do not participate in the davis vision. Please note that the member’s (or employee’s or authorized person’s).
In new hampshire, any person who, with a purpose to injure, defraud, or deceive any insurance company, files a statement of claim containing any false,. Use this form to request reimbursement for services received from providers who do not participate in the davis vision. Please submit claim reimbursement for each patient on a separate claim form. Vision care processing unit, p.o. The completion and submission of this form does. Box 1525, latham, ny 12110. Please note that the member’s (or employee’s or authorized person’s). Vision by metlife member reimbursement form to request reimbursement, complete and print this form, enclose a legible copy of your itemized. Mail completed claim form to:
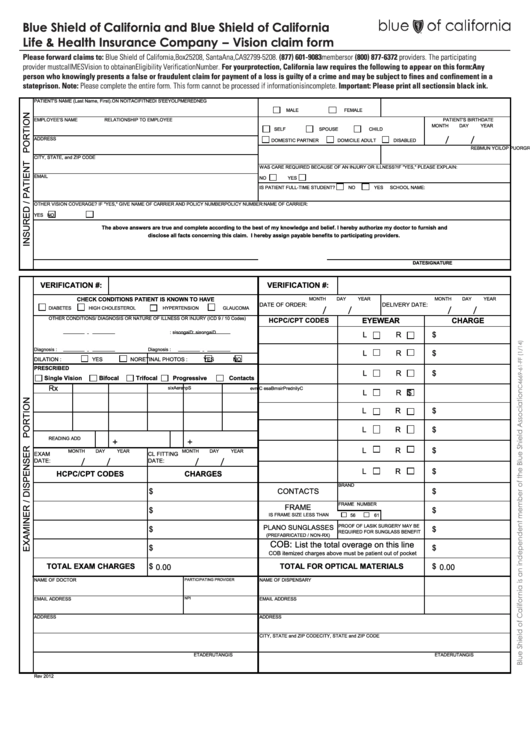
Fillable Vision Claim Form printable pdf download
Please submit claim reimbursement for each patient on a separate claim form. The completion and submission of this form does. Use this form to request reimbursement for services received from providers who do not participate in the davis vision. Vision by metlife member reimbursement form to request reimbursement, complete and print this form, enclose a legible copy of your itemized..
Top Davis Vision Claim Form Templates free to download in PDF format
Mail completed claim form to: Please note that the member’s (or employee’s or authorized person’s). Box 1525, latham, ny 12110. The completion and submission of this form does. Please submit claim reimbursement for each patient on a separate claim form.
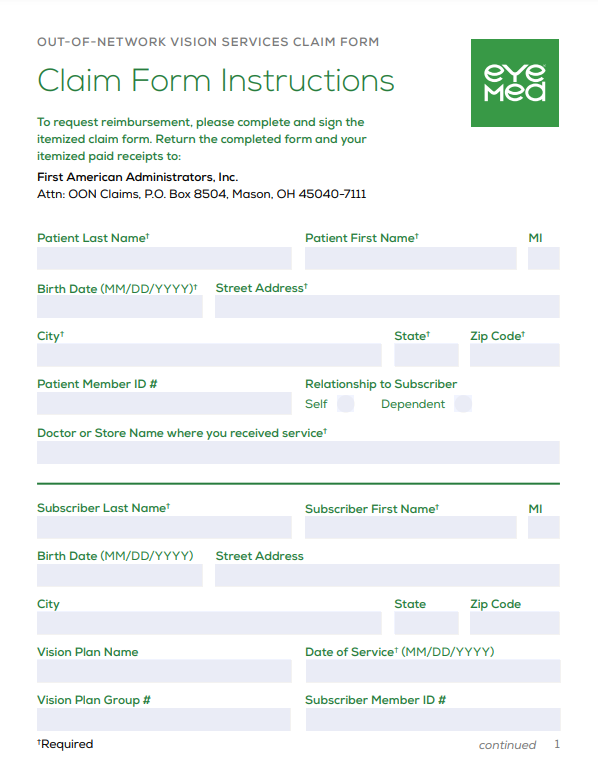
Eyemed Vision Care Reimbursement Form
Use this form to request reimbursement for services received from providers who do not participate in the davis vision. Box 1525, latham, ny 12110. The completion and submission of this form does. Please submit claim reimbursement for each patient on a separate claim form. Mail completed claim form to:
Davis Vision Form Fill Out And Sign Printable PDF Template SignNow
The completion and submission of this form does. Please note that the member’s (or employee’s or authorized person’s). In new hampshire, any person who, with a purpose to injure, defraud, or deceive any insurance company, files a statement of claim containing any false,. Vision by metlife member reimbursement form to request reimbursement, complete and print this form, enclose a legible.
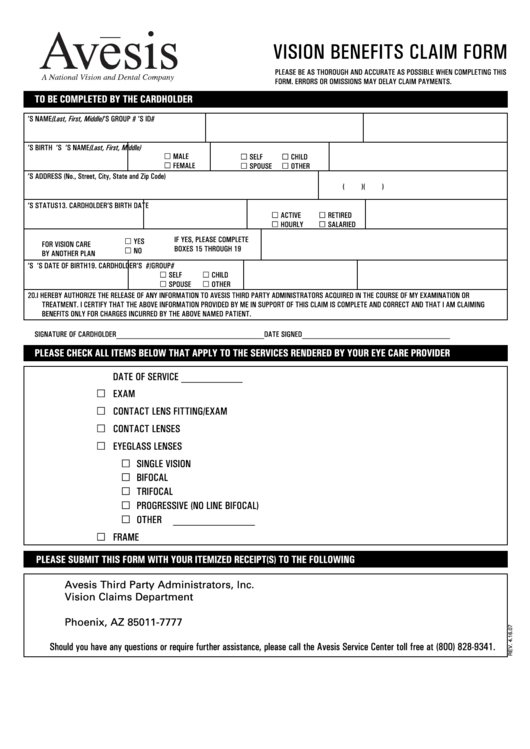
Fillable Vision Benefits Claim Form printable pdf download
Please note that the member’s (or employee’s or authorized person’s). Vision by metlife member reimbursement form to request reimbursement, complete and print this form, enclose a legible copy of your itemized. In new hampshire, any person who, with a purpose to injure, defraud, or deceive any insurance company, files a statement of claim containing any false,. Box 1525, latham, ny.

Vision Claim Form 2016 PDF
Please note that the member’s (or employee’s or authorized person’s). Please submit claim reimbursement for each patient on a separate claim form. Box 1525, latham, ny 12110. Mail completed claim form to: Vision care processing unit, p.o.

Always Care Vision Fill Online, Printable, Fillable, Blank pdfFiller
In new hampshire, any person who, with a purpose to injure, defraud, or deceive any insurance company, files a statement of claim containing any false,. Vision care processing unit, p.o. Box 1525, latham, ny 12110. Mail completed claim form to: The completion and submission of this form does.
Top Davis Vision Reimbursement Form Templates free to download in PDF
Please note that the member’s (or employee’s or authorized person’s). The completion and submission of this form does. Mail completed claim form to: Vision care processing unit, p.o. In new hampshire, any person who, with a purpose to injure, defraud, or deceive any insurance company, files a statement of claim containing any false,.

Claim Form Davis Vision Claim Form
Please submit claim reimbursement for each patient on a separate claim form. Vision care processing unit, p.o. In new hampshire, any person who, with a purpose to injure, defraud, or deceive any insurance company, files a statement of claim containing any false,. Use this form to request reimbursement for services received from providers who do not participate in the davis.

Fillable Online Davis Vision Out of Network Claim Form Fax Email Print
The completion and submission of this form does. Please submit claim reimbursement for each patient on a separate claim form. Mail completed claim form to: Vision by metlife member reimbursement form to request reimbursement, complete and print this form, enclose a legible copy of your itemized. Use this form to request reimbursement for services received from providers who do not.
Vision Care Processing Unit, P.o.
Mail completed claim form to: The completion and submission of this form does. Please note that the member’s (or employee’s or authorized person’s). Box 1525, latham, ny 12110.
In New Hampshire, Any Person Who, With A Purpose To Injure, Defraud, Or Deceive Any Insurance Company, Files A Statement Of Claim Containing Any False,.
Use this form to request reimbursement for services received from providers who do not participate in the davis vision. Please submit claim reimbursement for each patient on a separate claim form. Vision by metlife member reimbursement form to request reimbursement, complete and print this form, enclose a legible copy of your itemized.