Certification Of Health Care Provider Form - While use of this form is optional, this form asks the health care provider for the information necessary for a complete and sufficient medical. Documentation must be provided in english or be accompanied by a translation of medical. While use of this form is optional, this form asks the health care provider for the information necessary for a complete and sufficient medical. By the signature below, i give permission to my health care provider to clarify information regarding the clinical reason for me to take time from work. By the signature below, i give permission to my health care provider to clarify information regarding the clinical reason for me to take time from work. All medical facts must be provided by the treating provider.
By the signature below, i give permission to my health care provider to clarify information regarding the clinical reason for me to take time from work. All medical facts must be provided by the treating provider. By the signature below, i give permission to my health care provider to clarify information regarding the clinical reason for me to take time from work. While use of this form is optional, this form asks the health care provider for the information necessary for a complete and sufficient medical. While use of this form is optional, this form asks the health care provider for the information necessary for a complete and sufficient medical. Documentation must be provided in english or be accompanied by a translation of medical.
While use of this form is optional, this form asks the health care provider for the information necessary for a complete and sufficient medical. By the signature below, i give permission to my health care provider to clarify information regarding the clinical reason for me to take time from work. Documentation must be provided in english or be accompanied by a translation of medical. By the signature below, i give permission to my health care provider to clarify information regarding the clinical reason for me to take time from work. All medical facts must be provided by the treating provider. While use of this form is optional, this form asks the health care provider for the information necessary for a complete and sufficient medical.
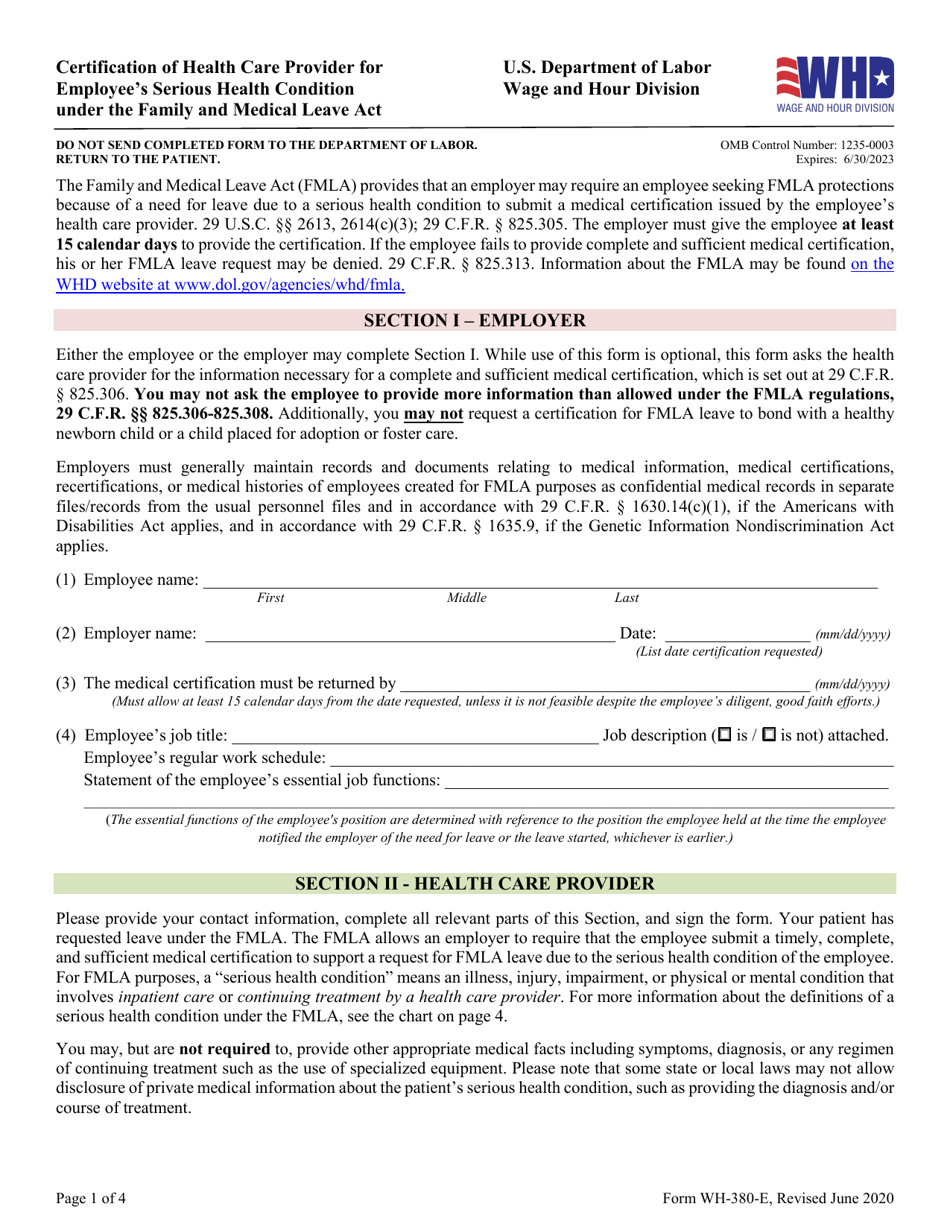
Form WH380E Download Fillable PDF or Fill Online Fmla Certification
All medical facts must be provided by the treating provider. While use of this form is optional, this form asks the health care provider for the information necessary for a complete and sufficient medical. By the signature below, i give permission to my health care provider to clarify information regarding the clinical reason for me to take time from work..

Certification Of Health Care Provider Form Fill Online, Printable
All medical facts must be provided by the treating provider. While use of this form is optional, this form asks the health care provider for the information necessary for a complete and sufficient medical. By the signature below, i give permission to my health care provider to clarify information regarding the clinical reason for me to take time from work..
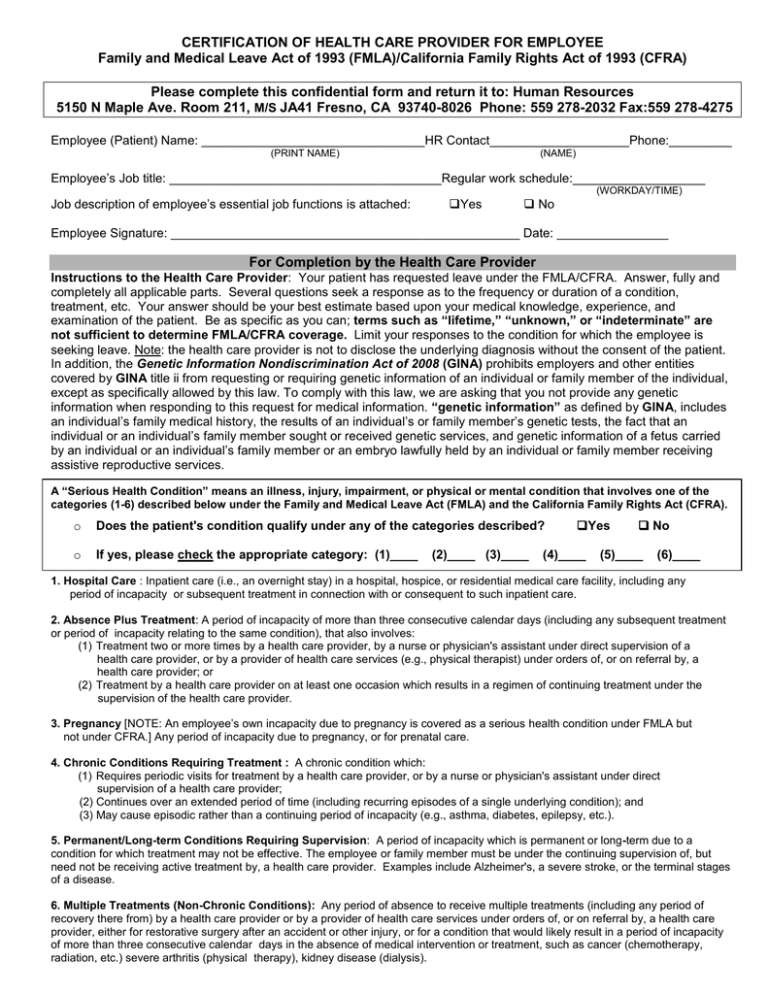
FMLA/CFRA Health Care Provider Certification Form
By the signature below, i give permission to my health care provider to clarify information regarding the clinical reason for me to take time from work. Documentation must be provided in english or be accompanied by a translation of medical. By the signature below, i give permission to my health care provider to clarify information regarding the clinical reason for.
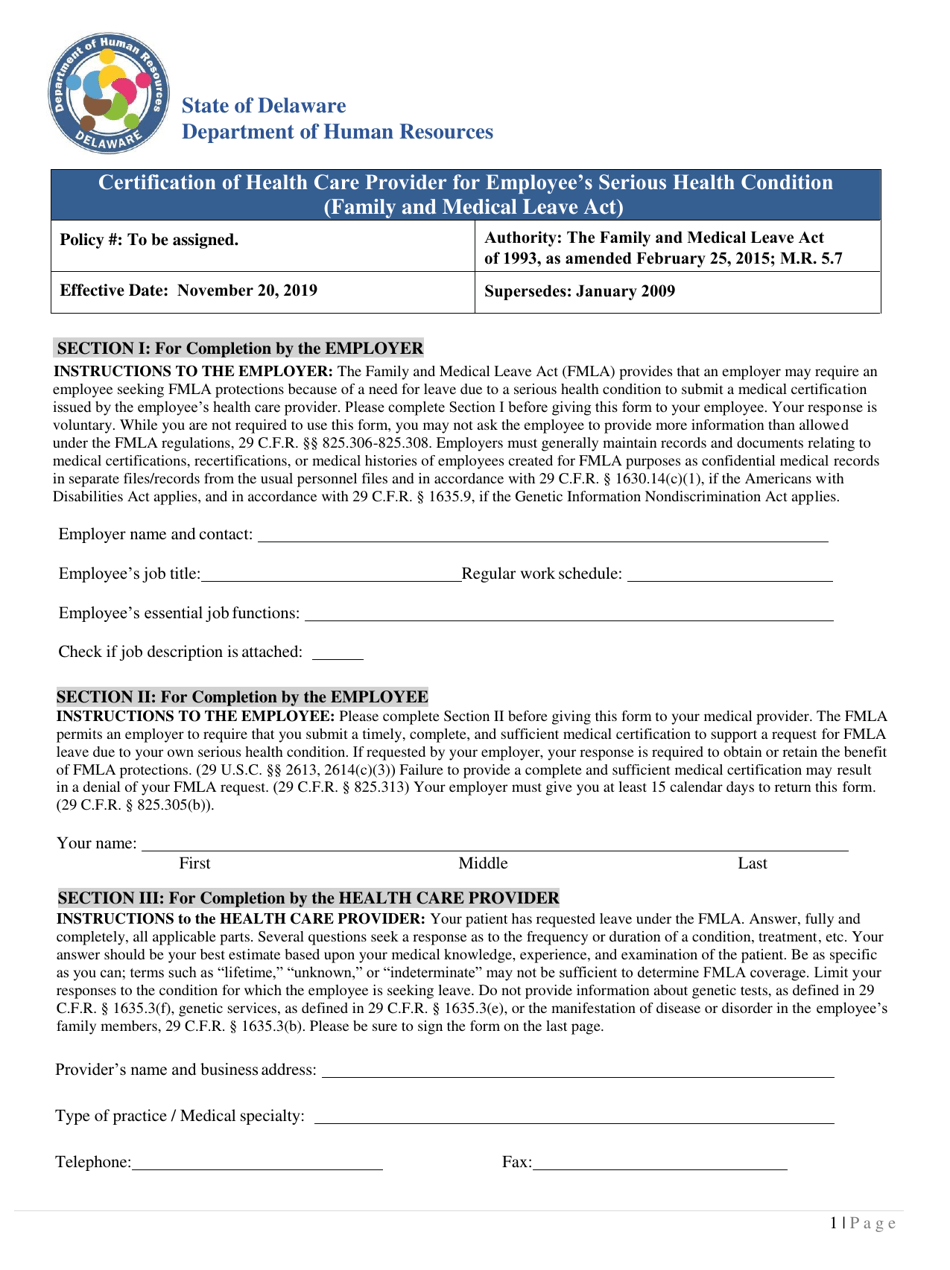
Delaware Fmla Certification of Health Care Provider for Employee's
All medical facts must be provided by the treating provider. By the signature below, i give permission to my health care provider to clarify information regarding the clinical reason for me to take time from work. While use of this form is optional, this form asks the health care provider for the information necessary for a complete and sufficient medical..

Certification of Health Care Provider for Employee's Doc Template
While use of this form is optional, this form asks the health care provider for the information necessary for a complete and sufficient medical. By the signature below, i give permission to my health care provider to clarify information regarding the clinical reason for me to take time from work. While use of this form is optional, this form asks.
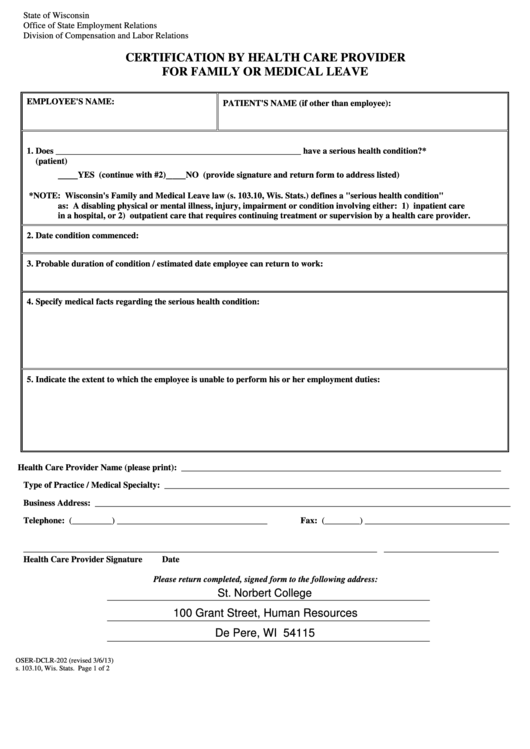
Fillable Certification By Health Care Provider For Family Or Medical
Documentation must be provided in english or be accompanied by a translation of medical. All medical facts must be provided by the treating provider. By the signature below, i give permission to my health care provider to clarify information regarding the clinical reason for me to take time from work. While use of this form is optional, this form asks.
2.jpg)
Unum Fmla Printable Forms
While use of this form is optional, this form asks the health care provider for the information necessary for a complete and sufficient medical. While use of this form is optional, this form asks the health care provider for the information necessary for a complete and sufficient medical. By the signature below, i give permission to my health care provider.
Fillable Form HcpcEml Certification Of Health Care Provider For
By the signature below, i give permission to my health care provider to clarify information regarding the clinical reason for me to take time from work. Documentation must be provided in english or be accompanied by a translation of medical. While use of this form is optional, this form asks the health care provider for the information necessary for a.
FMLA LEAVE CERTIFICATION OF HEALTH CARE PROVIDER SSN
By the signature below, i give permission to my health care provider to clarify information regarding the clinical reason for me to take time from work. While use of this form is optional, this form asks the health care provider for the information necessary for a complete and sufficient medical. While use of this form is optional, this form asks.
FAMU Family And Medical Leave Act (FMLA) Certification Of Health Care
While use of this form is optional, this form asks the health care provider for the information necessary for a complete and sufficient medical. All medical facts must be provided by the treating provider. By the signature below, i give permission to my health care provider to clarify information regarding the clinical reason for me to take time from work..
By The Signature Below, I Give Permission To My Health Care Provider To Clarify Information Regarding The Clinical Reason For Me To Take Time From Work.
By the signature below, i give permission to my health care provider to clarify information regarding the clinical reason for me to take time from work. While use of this form is optional, this form asks the health care provider for the information necessary for a complete and sufficient medical. While use of this form is optional, this form asks the health care provider for the information necessary for a complete and sufficient medical. All medical facts must be provided by the treating provider.